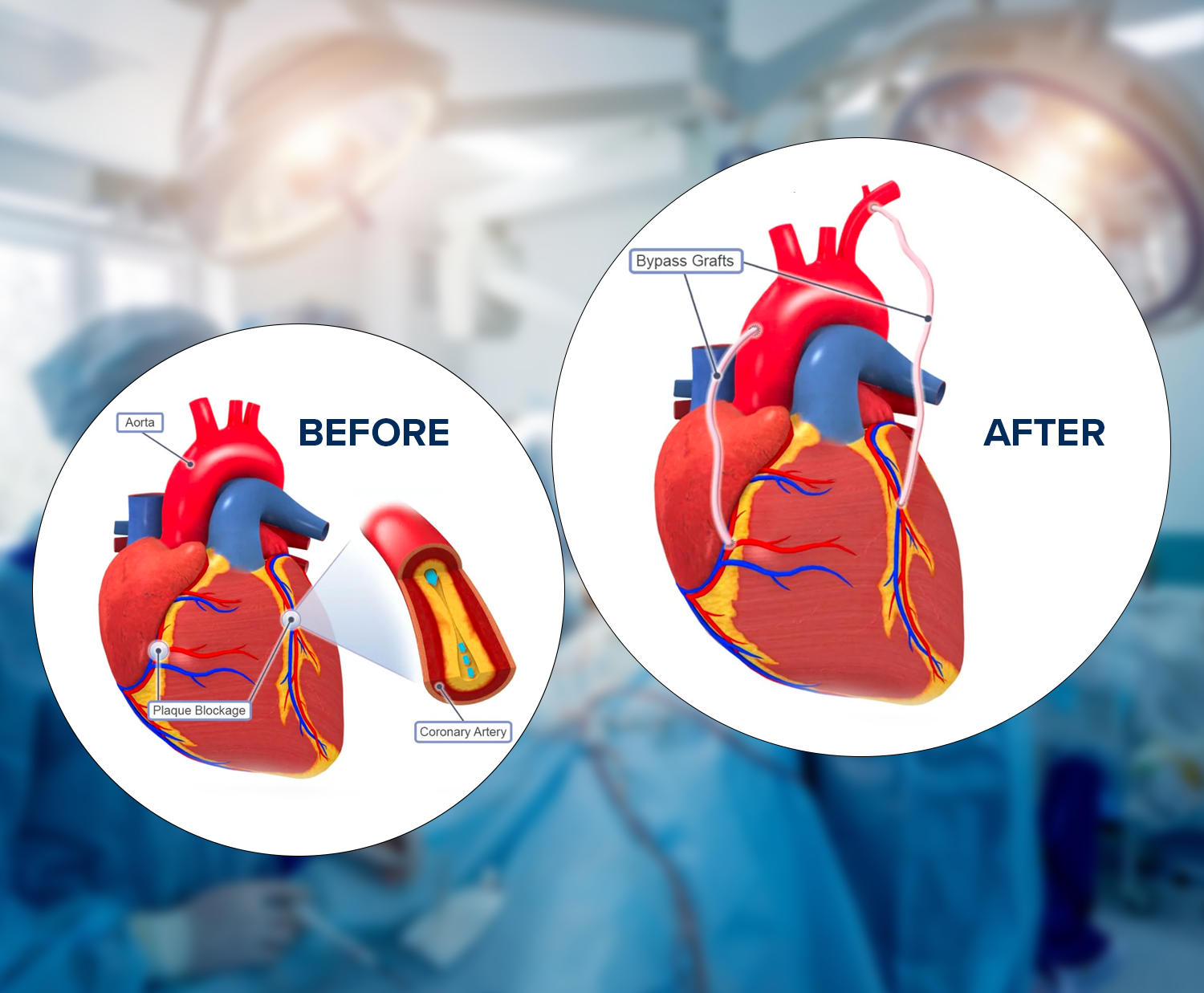
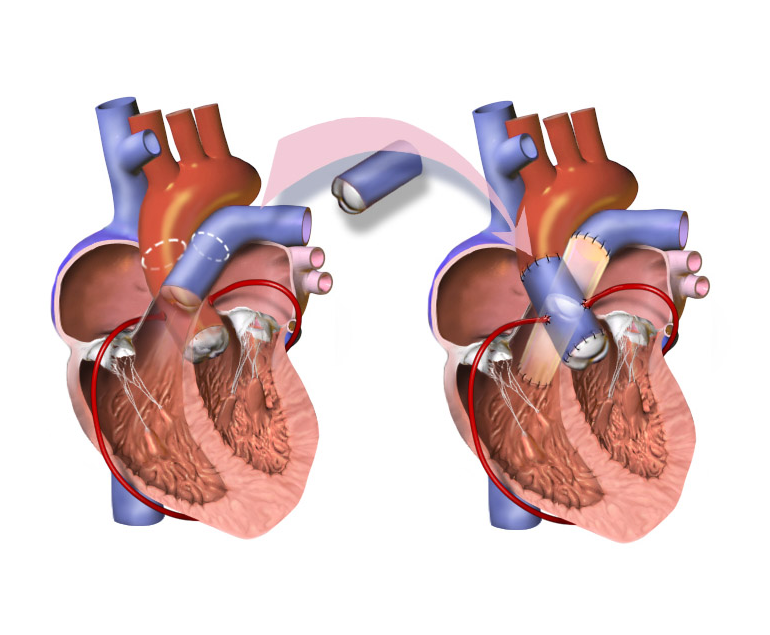
The psychological impact of undergoing Coronary Artery Bypass Grafting (CABG) surgery can vary from person to person, and factors such as individual resilience, pre-existing mental health conditions, and the presence of a strong support system can influence the experience. However, some common psychological effects may include:
- Anxiety and Fear:
• Preoperative anxiety is common, as individuals may be concerned about the surgery itself, potential complications, and the uncertainty of the outcome.
• Postoperative anxiety can occur due to concerns about recovery, lifestyle changes, and the future. - Depression:
• Some individuals may experience feelings of sadness or depression, often related to the impact of the surgery on their life, health, and well-being. - Body Image Concerns:
• Surgical scars, changes in appearance, and the perception of one’s body may lead to body image concerns, impacting self-esteem and emotional well-being. - Loss of Control:
• Surrendering control during the surgical process and depending on others for care can lead to a sense of vulnerability and loss of control, affecting emotional well-being. - Grief and loss:
• Individuals may experience grief and a sense of loss, particularly if they need to make significant lifestyle changes post-surgery or if they mourn aspects of their life prior to the surgery. - Coping with Pain:
• Postoperative pain can contribute to emotional distress, affecting mood and overall psychological well-being. - Social and Relationship Impact:
• Changes in health and lifestyle may impact social relationships. Some individuals may experience social isolation or changes in family dynamics, which can affect mental health. - Adjustment Challenges:
• Adapting to the post-surgery lifestyle, including medication regimens, dietary changes, and exercise requirements, can be challenging and may contribute to psychological stress. - Post-Traumatic Stress Disorder (PTSD):
• In some cases, individuals may develop symptoms of PTSD, especially if they experienced complications during or after the surgery. - Positive psychological changes:
• While there can be negative psychological effects, some individuals also report positive changes, such as increased appreciation for life, a reevaluation of priorities, and a focus on healthier living.
It’s important for healthcare providers to recognize and address the psychological impact of CABG surgery. Preoperative education, psychological support, and postoperative follow-up care are integral components of a comprehensive approach to ensuring not only physical recovery but also emotional well-being. Seeking support from mental health professionals, support groups, and loved ones can play a crucial role in helping individuals cope with the psychological aspects of CABG surgery.
The psychological impact of undergoing Coronary Artery Bypass Grafting (CABG) surgery can vary from person to person, and factors such as individual resilience, pre-existing mental health conditions, and the presence of a strong support system can influence the experience. However, some common psychological effects may include: