

News
Our News Section offers timely articles, breaking news, and expert insights on medical advancements, new treatments, and healthcare policies.
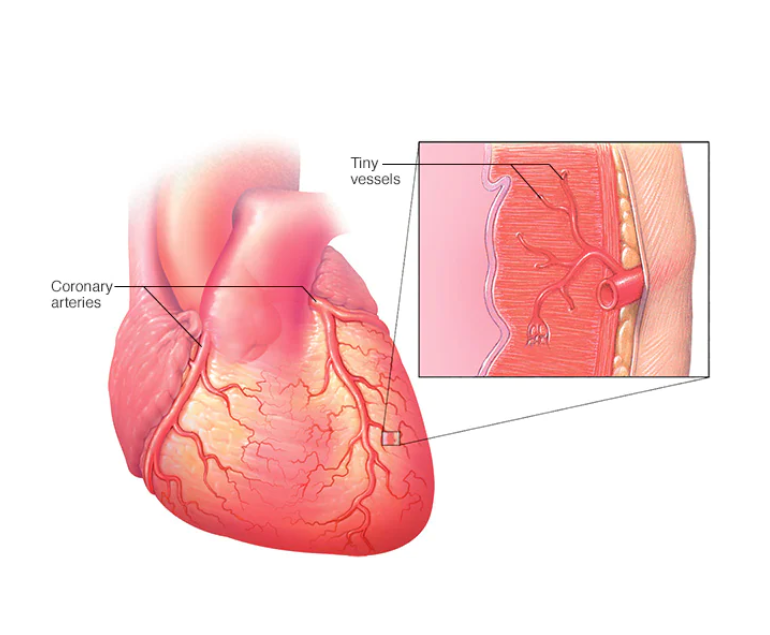
Coronary Microvascular Disease (CMD)
Coronary microvascular disease (CMD) is a condition that affects the small blood vessels in the heart. It is a common…
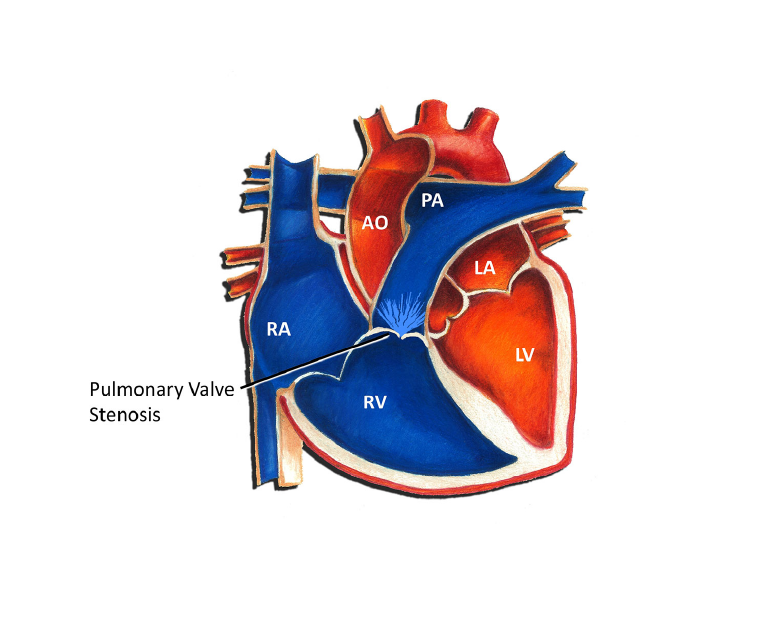
What is Pulmonary Valve Stenosis?
Pulmonary valve stenosis is a medical condition in which the pulmonary valve, which regulates blood flow from the right ventricle…

How Aerobic Exercise Keeps Heart Healthy
Aerobic exercise, also known as cardiovascular exercise, is any activity that raises your heart rate and increases your breathing for…
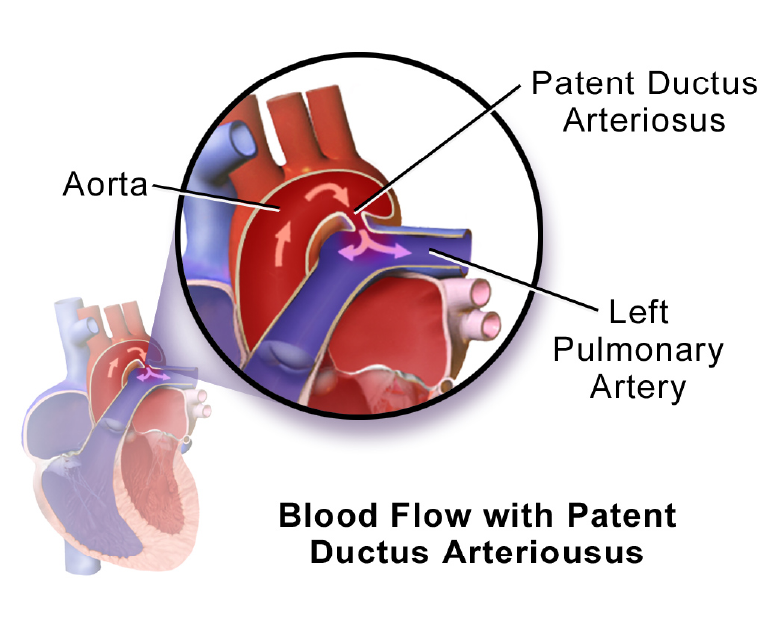
What is Patent Ductus Arteriosus (PDA) Defect?
Patent ductus arteriosus is a very common heart condition found in new born babies. It occurs because the ductus arteriosus…

How can Work Stress Hurt your Heart – and How to Prevent?
Stress is considered to be a normal part of life. Stress under manageable limits increases alertness and performance. However, uncontrolled…

Health Issues in Teenagers because of Breathing Polluted Air
Air pollution is very detrimental to human health. According to World Health Organization (WHO), air pollution is the reason for…
What is Acute Coronary Syndrome?
Acute coronary syndrome (ACS) refers to conditions where the blood supply to the heart muscle is suddenly blocked or severely…

An Overview of Breast Cancer
Breast cancer is the second most common cancer diagnosed in women. It occurs mostly in women, though men can also…
Women and Heart Disease
It is generally considered that heart disease affects men more than women. However, coronary heart disease is a leading cause…
What is Coronary Artery Disease?
Coronary artery disease (CAD) or coronary heart disease is a common type of heart disease that occurs when the arteries…

Life after Bypass Surgery
Coronary artery disease occurs due to the hardening of arteries supplying blood to the heart muscle. Bypass surgery is performed…
Signs and Symptoms of Omicron XE
The XE variant of Covid-19 is a mutation of Omicron BA.1 and BA.2 strains. It is a recombinant where two…

Heart Attacks Are Becoming Common In Young People
Heart attacks, which were once called “old man’s disease”, are now occurring more frequently in younger people including women. It…
How Depression and Heart Disease are interlinked?
Depression and heart disease are two widespread diseases observed among the general public today. They often occur simultaneously within the…
Effect of a Positive Mental State on Heart
Mental health is an important component of the overall health of an individual. It involves a combination of psychological, emotional,…