

News
Our News Section offers timely articles, breaking news, and expert insights on medical advancements, new treatments, and healthcare policies.
Rheumatic Heart Disease
Rheumatic heart disease (RHD) is a serious condition that affects the heart valves and is a result of complications from…

Cardiovascular Conditions in Older Patients
Cardiovascular conditions in older patients pose significant challenges due to the natural aging process and the increased prevalence of risk…
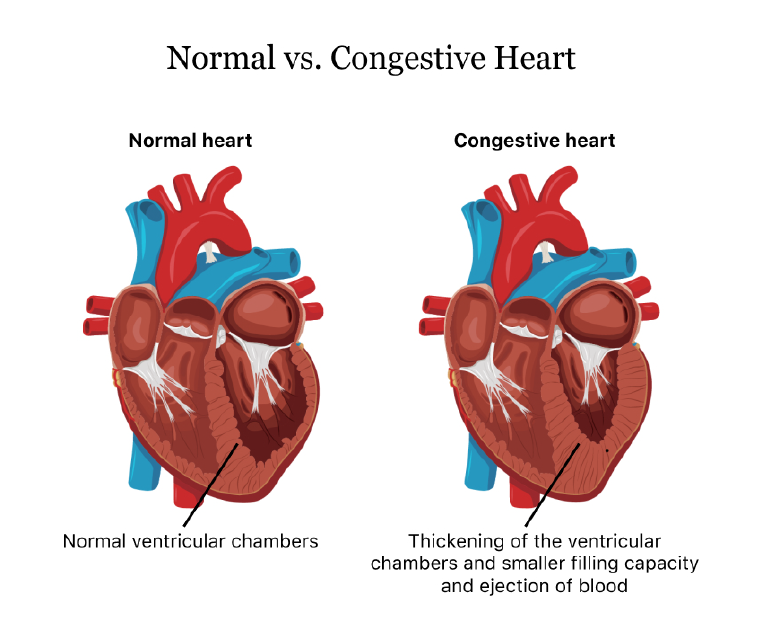
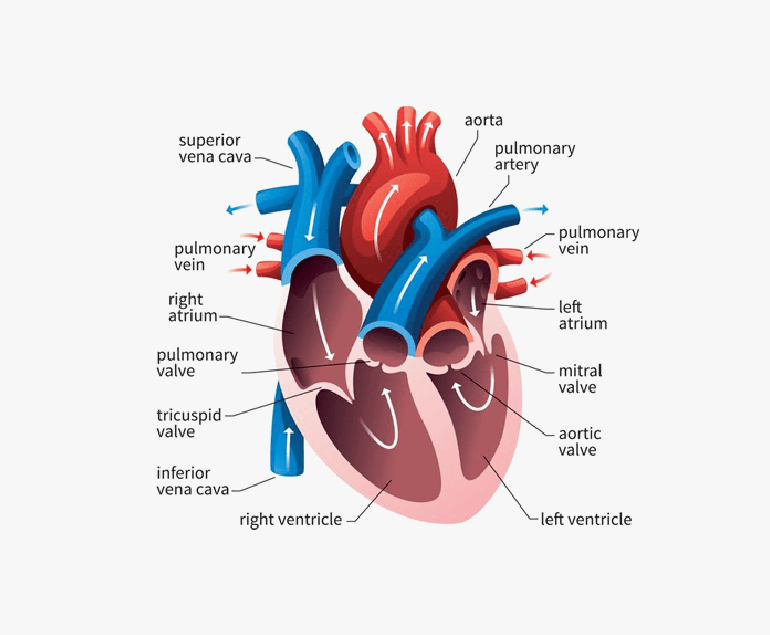
Congestive Heart Failure
Congestive heart failure (CHF) is a condition in which the heart is unable to pump blood effectively to meet the…

Dobutamine Stress Echocardiogram
Dobutamine Stress Echocardiogram, also known as DSE, is a non-invasive diagnostic test used to evaluate the function and blood flow…

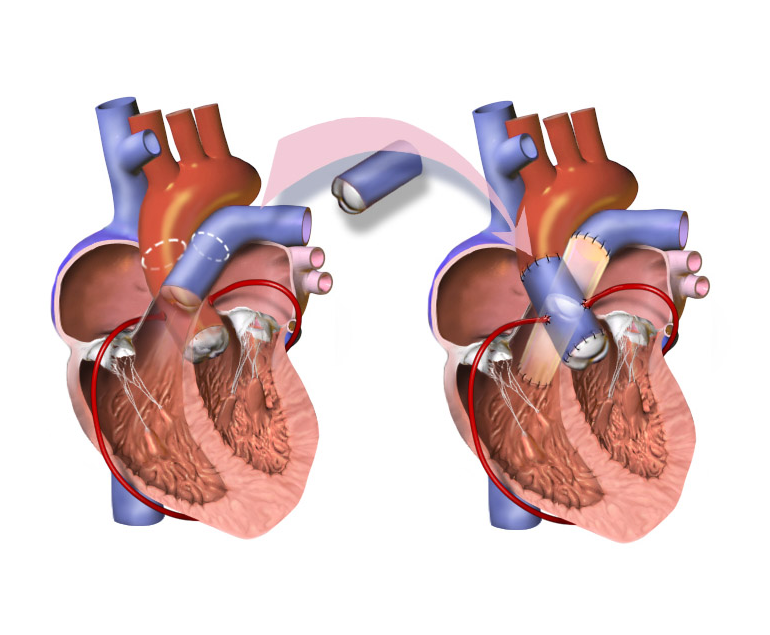
Pediatric Heart Transplant
Pediatric heart transplant is a complex surgical procedure that involves replacing a child’s damaged or diseased heart with a healthy…
Ross Procedure
The Ross procedure is a surgical procedure used to treat aortic valve disease, which is a condition in which the…
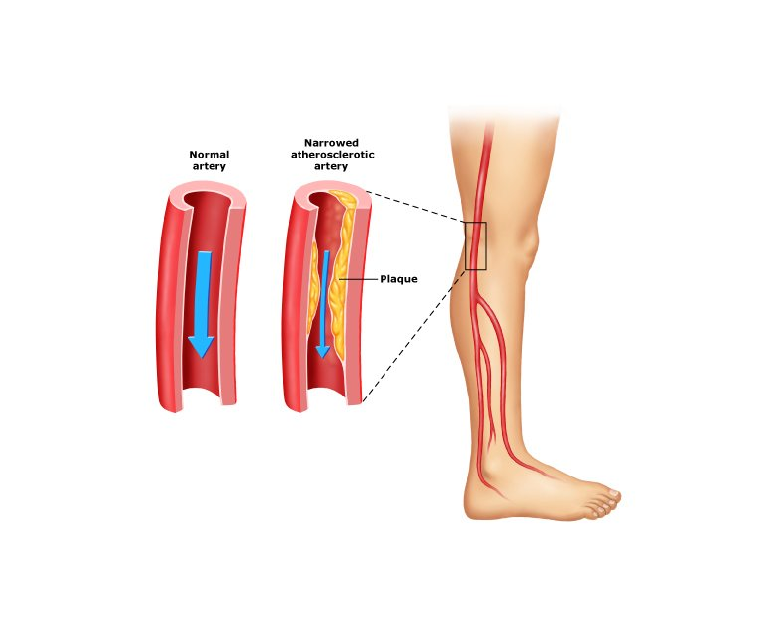
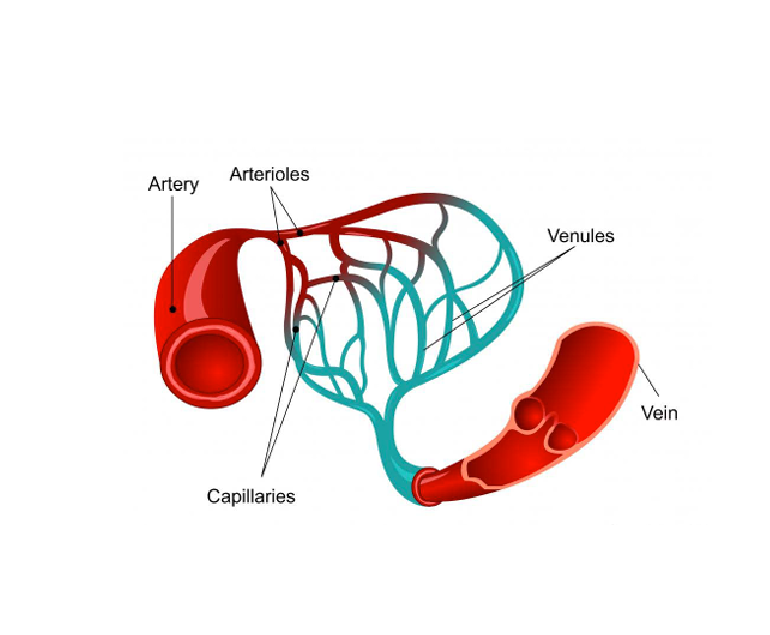
What is Peripheral Artery Disease?
Peripheral artery disease (PAD) is a circulatory condition that affects the peripheral arteries, which are the blood vessels that carry…
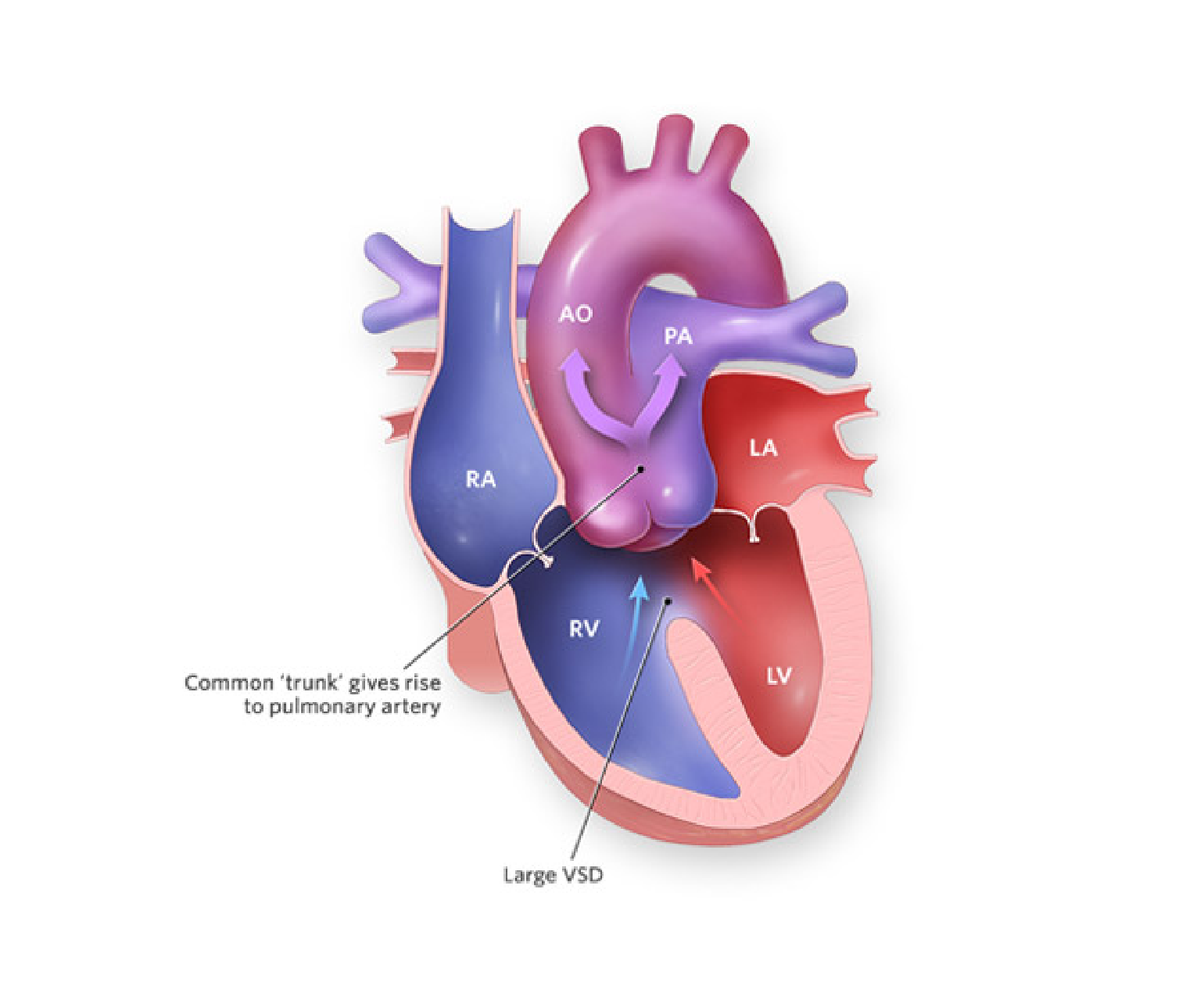
Truncus Arteriosus
Truncus arteriosus is a rare congenital heart defect that occurs in approximately 1 in 10,000 live births. It is a…
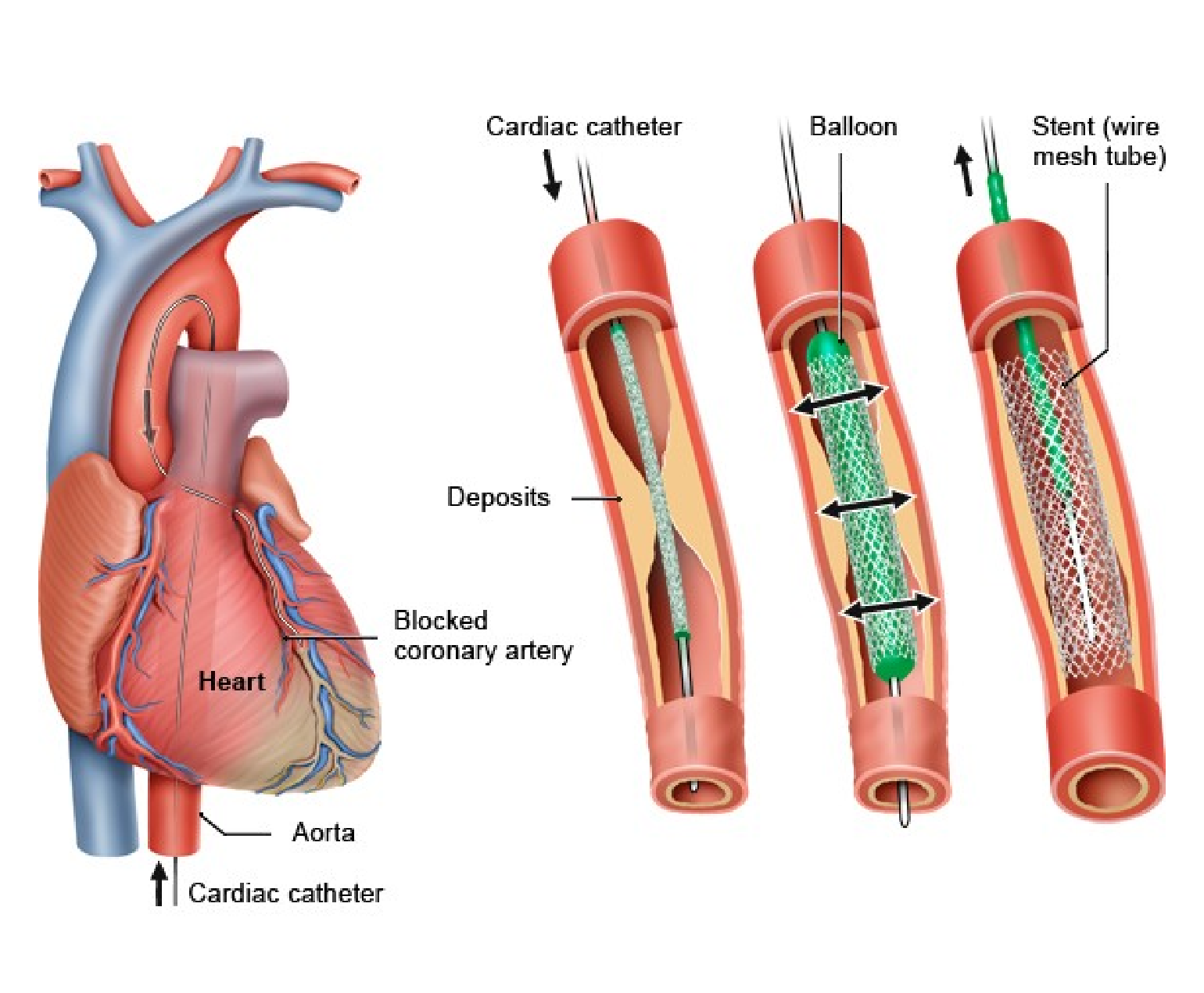
What is Cardiac Catheterization?
Cardiac catheterization, also known as coronary angiography, is a medical procedure that allows doctors to examine the heart and blood…

Electrical Cardioversion
Electrical cardioversion is a medical procedure that is used to treat abnormal heart rhythms, also known as arrhythmias. This procedure…
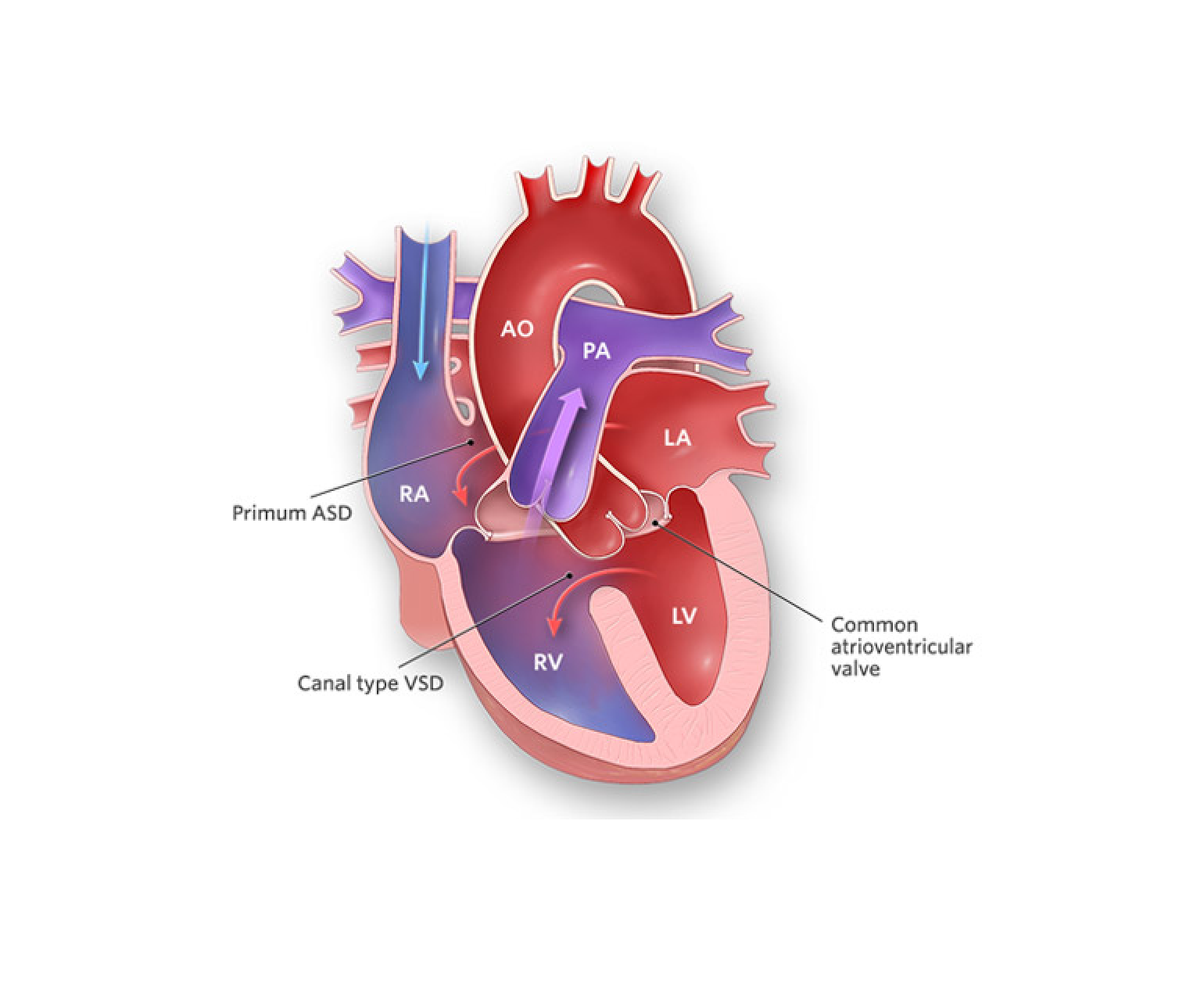
Complete Atrioventricular Canal Defect (CAVC)
Complete atrioventricular canal defect (CAVC) is a rare congenital heart condition that occurs when there is a hole in the…

How Positron Emission Tomography (PET) Scan Works?
Positron emission tomography (PET) is a medical imaging technique that produces detailed images of the inside of the body. It…
What is Vasculitis?
Vasculitis is a medical condition that affects the blood vessels in the body, leading to inflammation and damage to these…
Different Types of Heart Disease
Heart disease, also known as cardiovascular disease, refers to a range of conditions that affect the heart and blood vessels….
What is an Aortic Stenosis Murmur?
Aortic stenosis murmur is a heart condition characterized by a narrowed opening in the aortic valve, which is the valve…